

evidence & Applications
Cardiac Preservation and Prolonged Ischemic Storage
Donated hearts can be stored for up to four hours using static cold storage (SCS) – the accepted standard of care – before the risk of irreversible damage and primary graft failure rises sharply.
In an ongoing pig heart transplant study, static cold storage in Custodiol Solution (FDA-approved for cardiac preservation) for seven hours prior to transplantation resulted in severe ischemia-reperfusion injury, as indicated by impaired left ventricular wall motion (Fig. 1A, Left), significant reductions in ejection fraction (Fig 1B, Left), and decreased cardiac index (Fig 1C, Left) as measured two hours post-transplant and compared to pre-transplant baselines.
By contrast, static cold storage in Diatomic HTx Solution for seven hours prior to transplantation preserved pre-transplant cardiac function, as shown by normal left ventricular wall motion (Fig 1A, Right) and no loss in ejection fraction (Fig 1B, Right) or cardiac index (Fig 1C, Right) compared to pre-transplant baseline.
Our porcine cardiac transplant data promise the ability to safely extend the cardiac preservation time limit from the current standard of care (four hours) to a new standard of care (seven hours) using Diatomic HTx Solution.
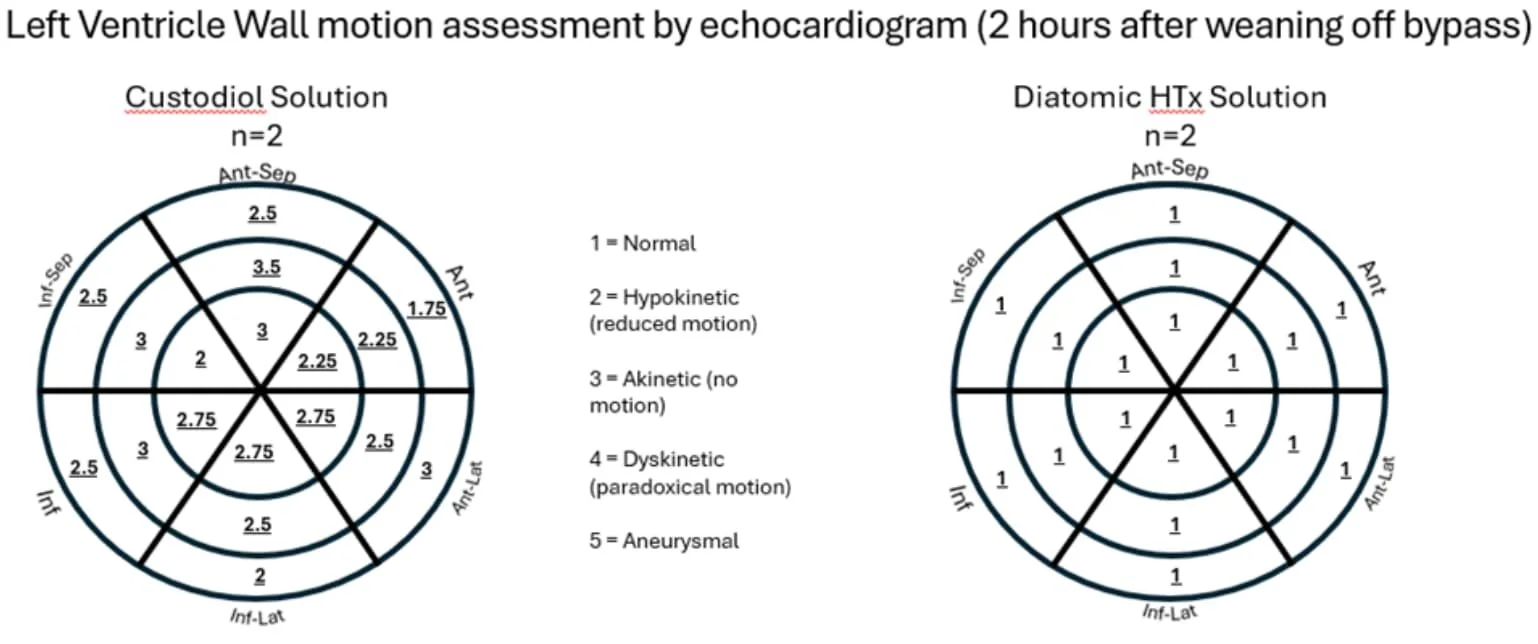
FIG. 1A

FIG. 1B
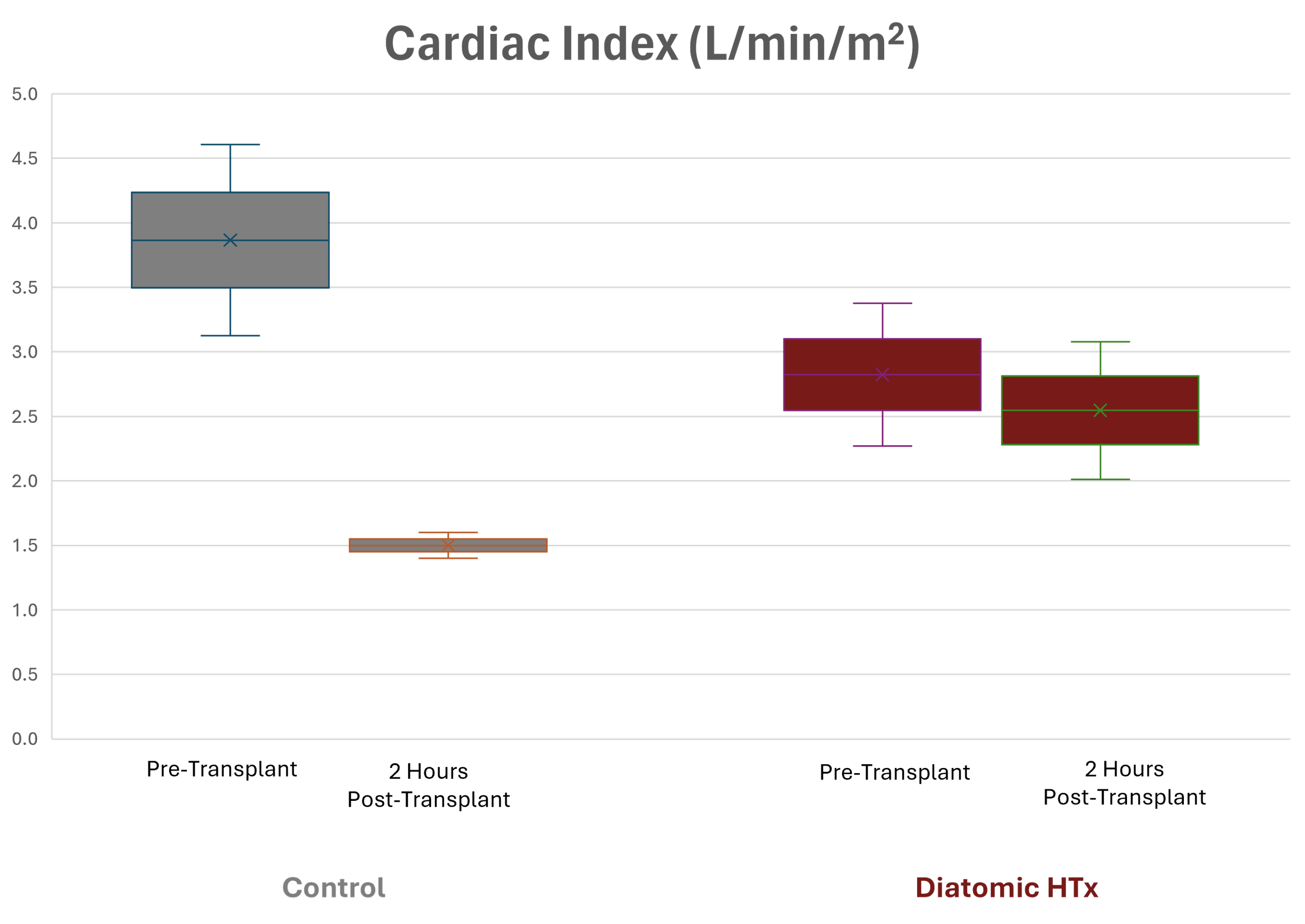
FIG. 1C
DCD Kidney Preservation with 50% Reduction in Reperfusion Injury Versus Standard of Care
For kidneys donated after cardiac death (DCD), hypothermic ex vivo machine perfusion prior to transplantation is the accepted standard of care. Even with the benefits of hypothermic ex vivo machine perfusion, reperfusion injury remains a major factor contributing to increased costs, delayed graft function, prolonged hospital stays, and long-term transplant complications.
In a porcine DCD kidney transplant study, we compared the current standard of care (flushing with UW solution and perfusing with Belzer MPS solution) to a new preservation protocol using H2-enhanced solutions (modified UW+H2 and Belzer MPS+H2 solutions) for flushing and perfusion. Six kidneys were used in each arm of the study.
Kidneys treated with the H2-enhanced UW and Belzer MPS solutions showed significantly improved functional recovery, as indicated by increased urine output, lower vascular resistance, and higher creatinine clearance rates (Fig 2, E-K).
In histopathology and immunostaining analyses, the hydrogen-protected kidneys exhibited significantly reduced reperfusion injury, as evidenced by lower scores for acute tubular necrosis (ATN) and reduced immunohistochemistry (IHC) staining for kidney injury marker (KIM-1), inflammation markers IL-6 and CD68, oxidative stress markers MPO and MDA, and TUNEL staining for apoptosis (Fig 3, A-H).
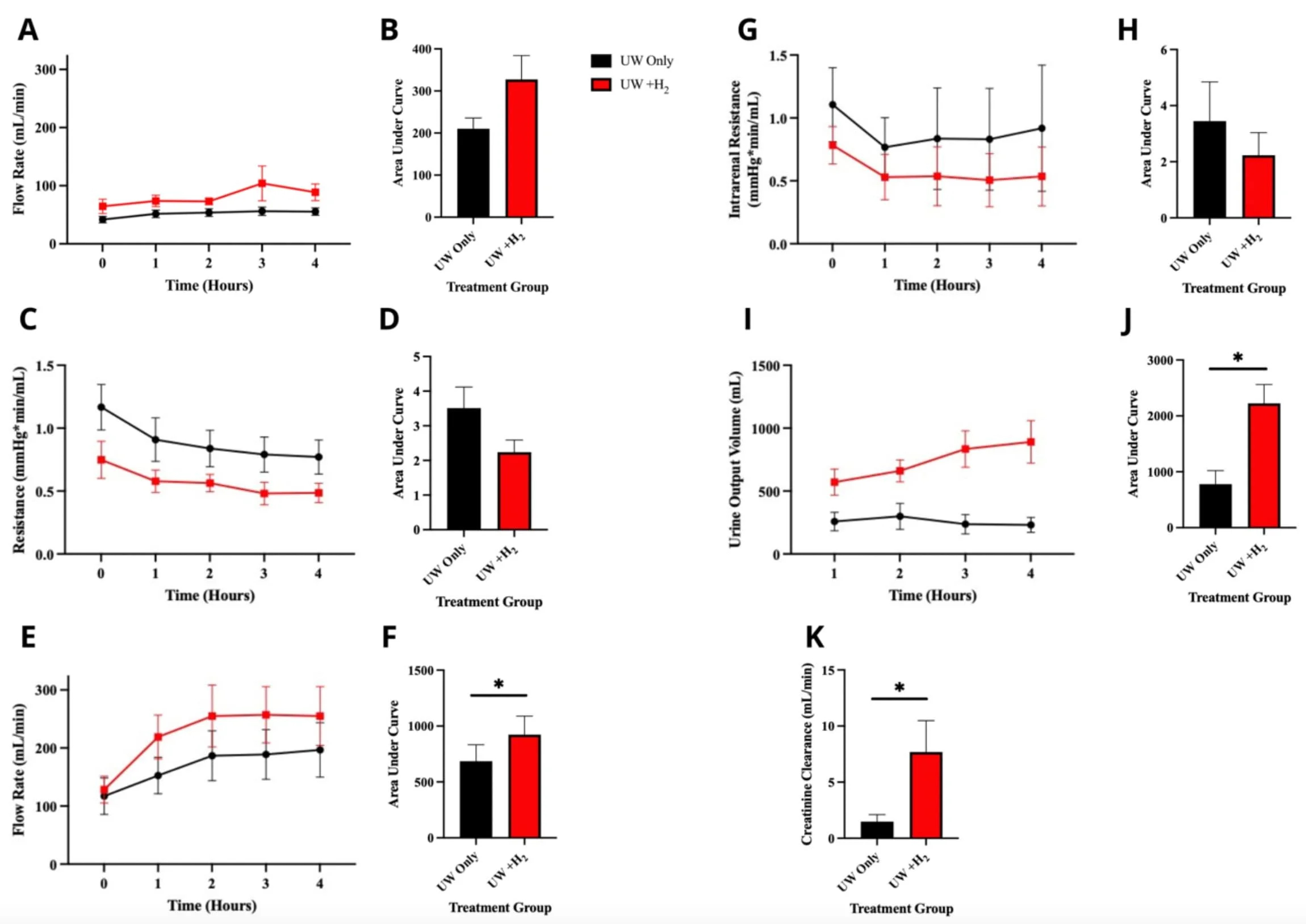
Figure 2. UW+H2 improves physiological functions of renal grafts. Mean hourly perfusate flow (A) and resistance (C) rates for UW+H2 (n=6) and UW-only (n=6) kidneys during cold storage. Mean hourly blood flow (E) and intrarenal resistance (G) rates, as well as urine output (I) throughout reperfusion between UW+H2 and UW-only treated grafts. Creatinine clearance during the first hour of reperfusion by UW+H2 and UW-only kidneys (K). Mean area under the curve (AUC) analyses of parameters between treatment groups based on corresponding time-course data; specifically, AUC values represent grafts' cumulative urine output (J), as well as perfusate and blood flow rates (B, F, respectively) and intrarenal resistance rates (D, H) during storage or reperfusion, respectively. AUCs were compared between treatment groups to assess differences in renal function and significance determined using paired T-tests. Black dots/bars represent UW-only group while red squares/bars represent UW+H2 group; error bars indicate± SEM. * p < 0.05.
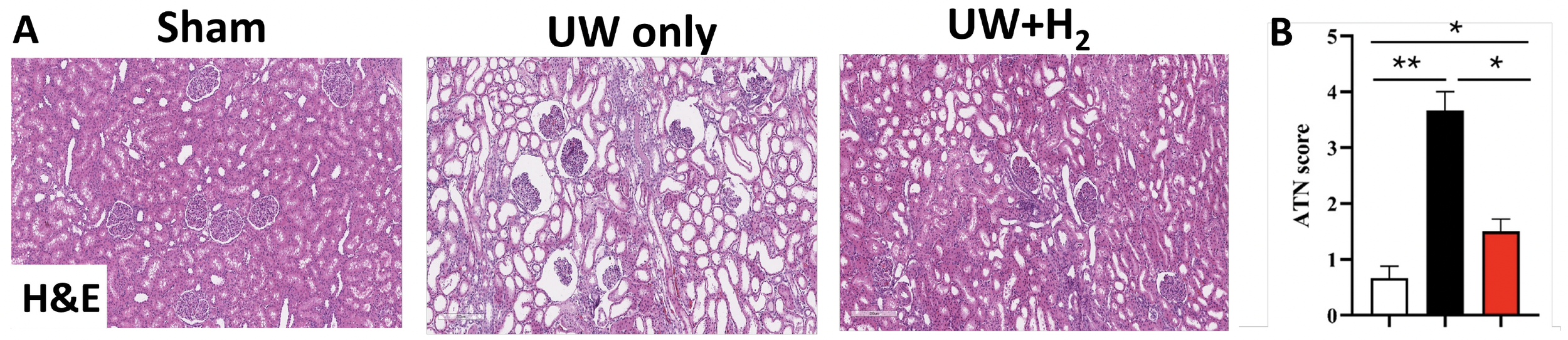
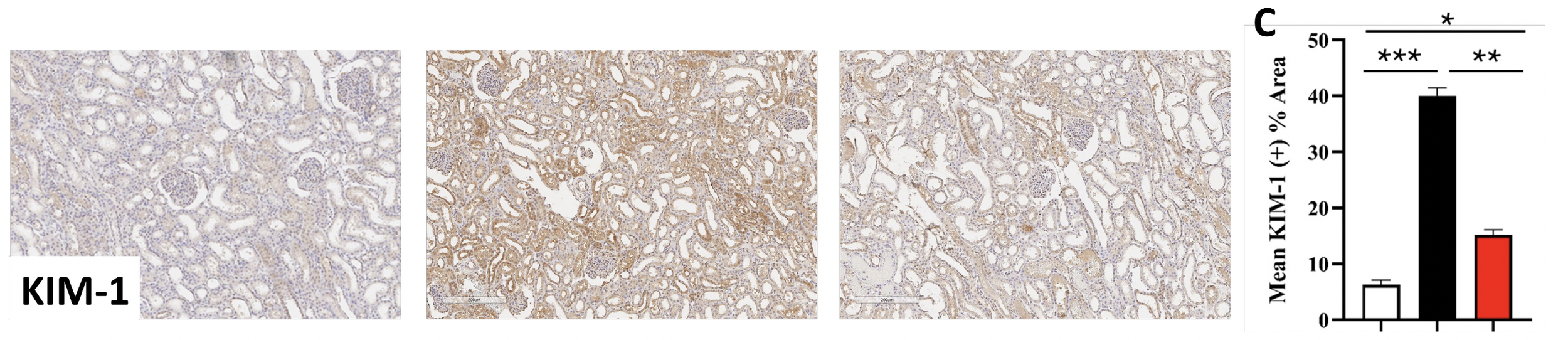
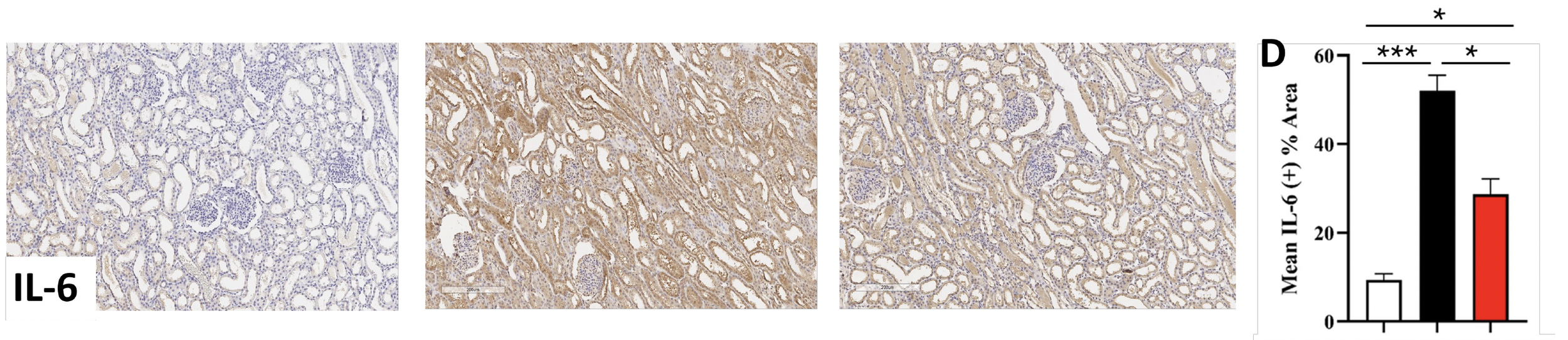
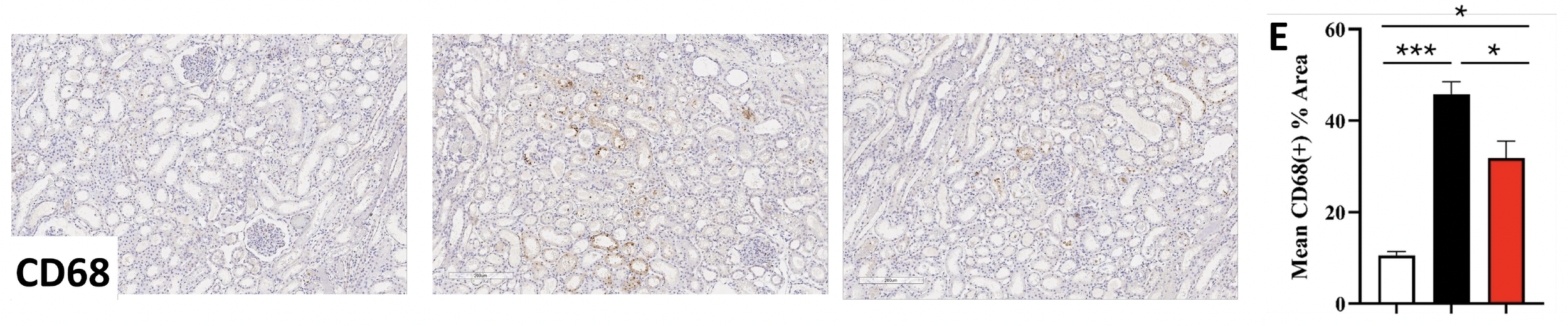
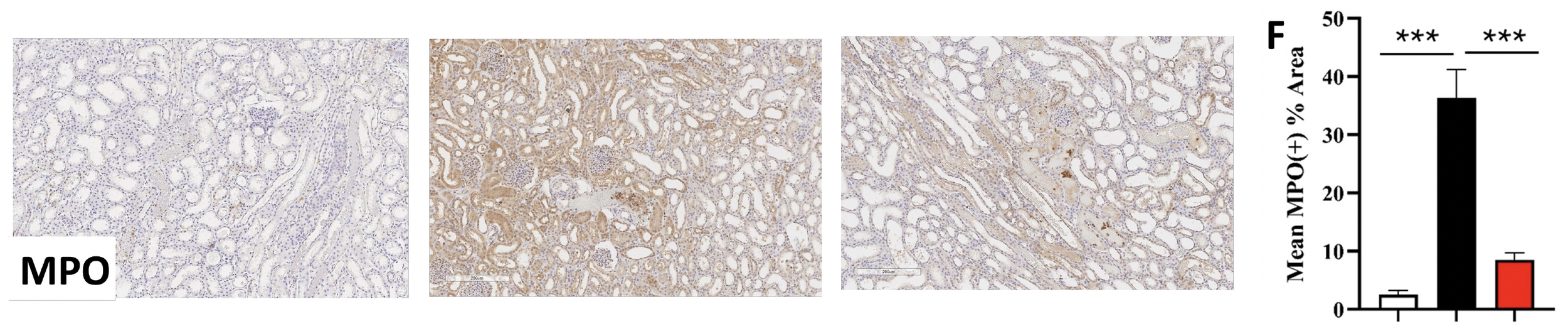
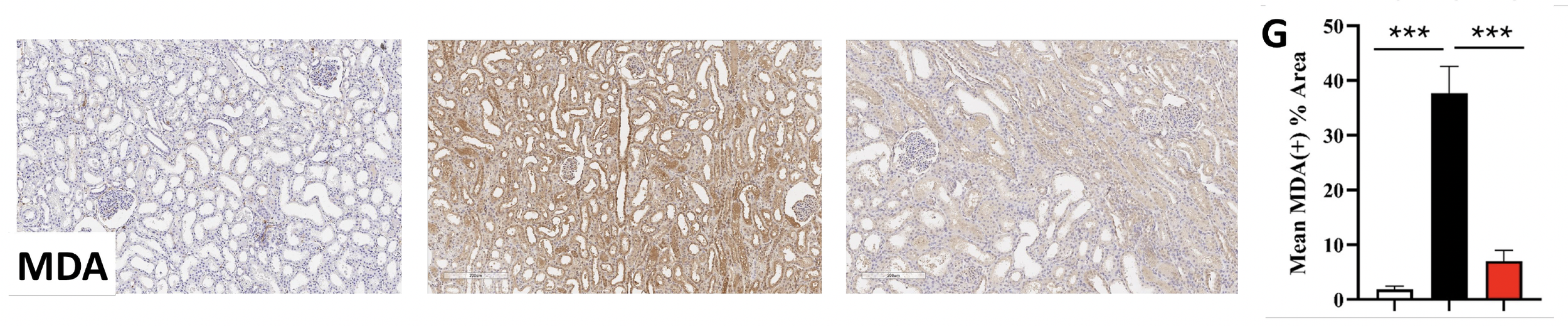
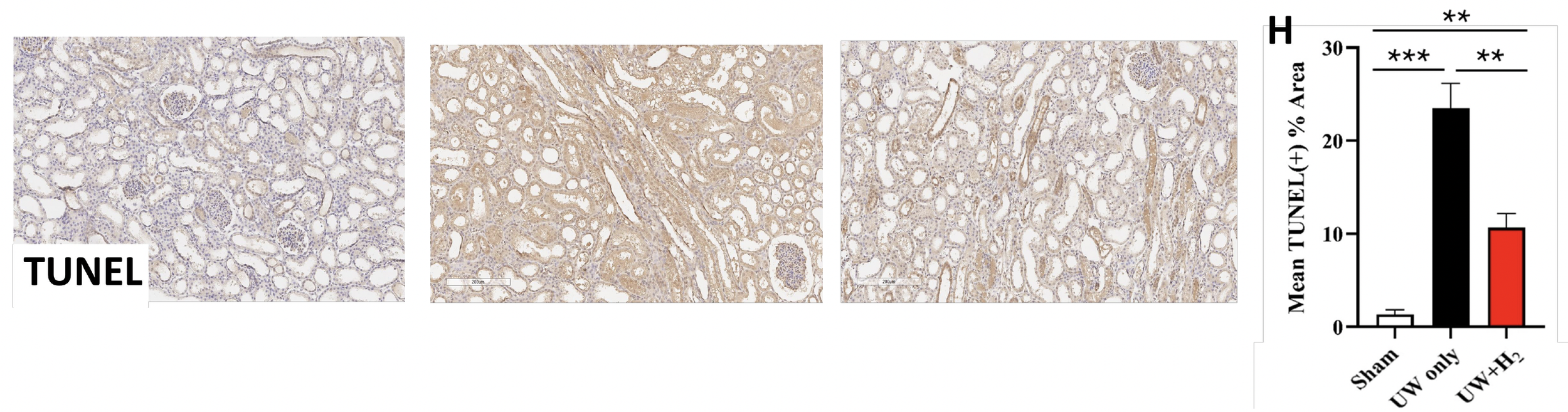
Figure 3. UW+H2 administration has protective effect against renal graft injury following reperfusion. Representative images (A) and quantitative analysis of acute tubular necrosis (ATN) score (B), KIM-1 expression (C), IL-6 expression (D), CD68 expression (E), MPO expression (F), MDA expression (G), and apoptosis of renal cells (H) following immunohistochemical staining of UW+H2 treated (n=6), UW-only treated (n=6), and sham kidney sections (n=6). Bars represent mean score and significance between groups determined using paired T-tests. Error bars indicate ± SEM. * p < 0.05, ** p < 0.01, *** p < 0.001.